
Sean provides guidance on how best to understand the different ways depression can present and the best principles and practices that can guide treatment planning, including when to refer to specialist care.
What is depression?
As GPs in Ireland, you often provide the first opportunity for patients to be diagnosed with depression. You act as the primary, central point of access for mental health support, offering assessments, referrals and treatment plans for issues like anxiety and depression. GPs often provide the most enduring support for people living with depression.
Depression is more than normal sadness or stress response which affects mood, thinking, physical health and behaviour. The core symptoms of depression, according to the DSM-5, must include depressed mood OR loss of interest/pleasure, plus three or four of the following:
- Sleep disturbance
- Appetite/weight change
- Fatigue, low energy
- Poor concentration
- Feelings of guilt/worthlessness
- Psychomotor change
- Suicidal ideation.
Major depressive disorder requires symptoms to be persistent for more than two weeks with significant functional impairment. Symptoms cannot be caused by substances or better explained by another medical condition. Symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Depression sub-types with specific presentations include:
- Major depressive disorder
- Persistent depressive disorder / dysthymia
- Recurrent depression
- Perinatal / postnatal depression
- Depression with psychotic features
- Bipolar depression (important to avoid misdiagnosis).
Supporting patients with depression is aided through careful assessment, seeking collateral information, establishing and maintaining links with referral and support services and providing education and support to patients and their families.
Approaching conversations about depression and low mood with patients
When trying to identify and diagnose depression in a busy GP clinic, it can help to slow down or, in the first 60 seconds, to try to observe and notice your patient’s presentation without assumption. It may be helpful to ask explicitly about low mood without judgement; to reassure about time if patients fear “burdening” their GP; and to respond with compassion and validation to aid rapport and trust- building.
Patient-centred communication is fostered by creating a safe disclosure environment through warmth, patience and empathy, signalling safety early; patients decide within seconds that they feel safe to disclose emotional distress.
It is important to ask about suicide risk directly and take immediate action if high-risk of harm is identified, with an urgent referral or emergency department referral and safety planning. Patients rarely offer this information voluntarily and helpful questions that you can ask may include “over the past two weeks, have you experienced:
- Thoughts of being better off dead?
- Thoughts of harming themselves?
- Any plan or preparation?
- What has stopped you from acting on these thoughts/plans to end your life?”
When assessing functional impact, which is an important severity marker of depression, it can help to ask about work performance, absenteeism, social withdrawal, and quality of relationships and self-care.
Challenges to diagnosing depression
There can be challenges to accurately diagnosis depression as two‑thirds of patients may present to GPs with physical symptoms only, such as fatigue, sleep problems, headaches, chronic pain and gastrointestinal symptoms.
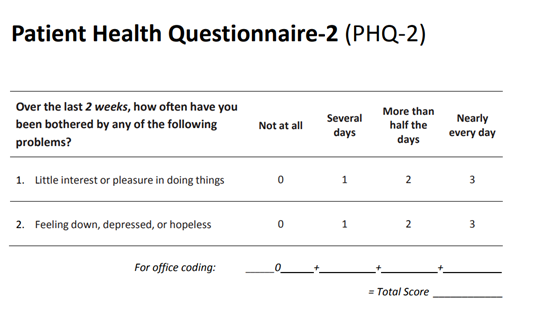
If you suspect your patient may be depressed the two Patient Health Questionnaire-2 (PHQ2) questions outlined in the table below can help explore this. Ask your patient “over the past two weeks, how often have you been bothered by any of the following problems: feeling down, depressed or hopeless; and little interest or pleasure in doing things”.
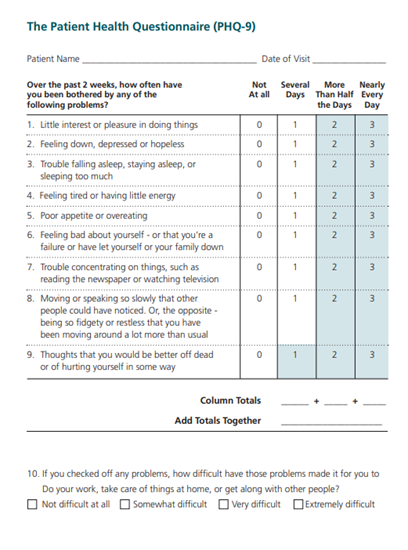
The PHQ9 assessment scale can also help clarify if patients’ symptoms may be related to depression.
Bipolar disorder and psychosis symptoms
If depression symptoms are identified, it is important to assess if your patient has experienced hypomania or mania symptoms in the past and/or psychosis symptoms.
Ante and postnatal depression
The World Health Organisation (WHO) describes a high prevalence of antenatal and postnatal depression of between 10% and 13%. This makes early diagnosis and treatment a high priority for the wellbeing of the mother, child and family unit.
Specific, sensitively asked questions can include:
- If the patient is having any difficulties caring for herself or the baby
- If the patient experiences any intrusive thoughts about harming herself or the baby.
These questions can help identify if depression may be present. If ante/postnatal depression is diagnosed, consider psychotherapy first and, if prescribing medication, sertraline is preferred.
Depression in older adults
Older adults often present with more somatic symptoms, sleep disturbances and anxiety symptoms. Some 60 to 70% of people with dementia experience symptoms of depression and/or anxiety, therefore considering assessment of cognitive impairment versus depression using the Mini-Mental State Examination (MMSE) may be indicated.
Depression, insomnia and sleep disorders
Sleep and depression have a strong bidirectional relationship. Insomnia doubles the risk of developing depression. Treating sleep disorders improves mood, functioning and relapse prevention.
Common sleep disorders to rule out include insomnia disorder, sleep apnoea, parasomnias and hypersomnia. If a specific sleep disorder is indicated, specialist referral pathways in Ireland include:
- Sleep clinics (Beaumont Hospital, ResMed, PEI, Bon Secours, Mater Private)
- An eight-week Cognitive Behavioural Therapy for Insomnia programme for psychological treatment of insomnia here in SPMHS, to which GPs can directly refer.
When to refer patients presenting with depression to specialist services
Follow the National Institute of clinical excellence (NICE) guidelines:
- Step 1: Assessment, referral, psychoeducation, monitoring and support.
- Step 2: Low-intensity therapy for mild depression.
- Step 3: Anti-depressants + high-intensity therapy for moderate to severe depression.
- Step 4: Specialist care for complex, high-risk, psychotic or treatment-resistant depression.
Referral options include:
- GP → Community mental health team
- GP → Primary care psychology (where available)
- GP → Counselling in primary care
- GP → Specialist perinatal mental health services
- GP → Private psychology/CBT therapists
Urgent versus routine referrals to specialist mental health services
GPs can make an urgent referral if there is:
- High suicide risk
- Psychotic symptoms
- Severe functional decline
- Severe agitation or mania
- Pregnancy/postnatal depression with moderate to severe symptoms.
GPs can make a routine referral if there is:
- Treatment-resistant depression
- Diagnostic uncertainty
- Comorbid substance misuse.
If you identify treatment-resistant depression, which you might suspect when there has been no response after two adequate trials of anti-depressants, it may be helpful to consider:
- Reassessing the diagnosis (bipolar disorder? substance use?)
- Assess what the therapeutic optimal dose for your patient is
- Switch/augment anti-depressant
- Add psychotherapy
- Referral to specialist mental health services.
Day programmes and cognitive behavioural therapy (CBT)
St Patrick’s Mental Health Services provides a Depression Recovery Programme and Bipolar Recovery programme, as well as a range of other day programmes GPs can refer directly to. Learn more here.
CBT can be accessed via St Patrick’s Mental Health Services. Complete a referral form and send to referrals@stpatricks.ie (Dean Clinic outpatient: Four to six weeks to review for suitability).
There are also HSE/community mental health team CBT provisions dependent on the county. CIPC/NCS for mild–moderate presentations. More information here.
The following websites list private accredited therapists:
- Cognitive Behavioural Psychotherapy Ireland
- Irish Association for Counselling and Psychotherapy
- Irish Association of Humanistic and Integrative Psychotherapy.
Other supports
- Aware support groups (online and in-person)
- Pieta (crisis support for suicide and self-harm)
- Mental Health Reform (Map of local services)
- Recovery College resources
- HSE YourMentalHealth.ie line: 1800 111 888
- Jigsaw (aged 12-25 yrs)
- Rotunda perinatal mental health supports
- PHQ‑9 Microsoft Word - PHQ9.doc
- NICE NG222 Overview | Depression in adults: treatment and management | Guidance | NICE
- National Maternity Hospital perinatal mental health service.
Summary
Depression is common and often presents somatically.
Making your consultation approach compassionate, open and sensitive to the needs of patients presenting with depression can help aid diagnosis and effective intervention.
The PHQ‑2/PHQ‑9 are practical tools for aiding diagnosis and monitoring. It is important to match the treatment step to severity and treatment response; it is often helpful to combine medications and therapy for best outcomes.
Always assess suicide risk directly and be familiar with local and national referral options. Early intervention improves outcomes and reduces suicide risk.
Recommended treatments for mild depression include:
- Monitoring symptoms
- Behavioural activation (activity scheduling)
- Guided self‑help (CCI Self-Help )
- Online CBT (SilverCloud, etc.)
- Exercise programmes (National Physical Activity and Sedentary Guidelines for Ireland)
Recommended treatments for moderate depression include:
- Prescribe SSRI as first-line antidepressant (ADT)
- CBT / Interpersonal psychotherapy (IPT) / Behavioural activation (BA) referral
- Lifestyle interventions continue
- Review in two to three weeks
- Use PHQ‑9 to track improvement.
Recommended treatments for severe depression include:
- Prescribe SSRI or Serotonin and Norepinephrine Reuptake Inhibitors (SNRI)
- Consider combination with therapy
- Safety planning
- Regular monitoring
- Assess for bipolar symptoms.